Optician / Keeler Case Study Competition 2010
Entry for : Ronnie MacGregor - Stranraer
email : r.macgregor@nhs.net
Click on any Thumbnail Image to see it full size.
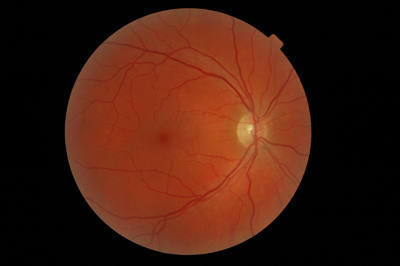
Routine Digital Retinal Imaging (DRI)
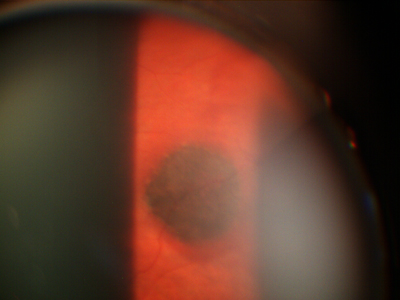
This 45 degree central field image of the Right Eye is typical of routine captures, taken with one of our Topcon TRC-NW6S machines, fitted with a Nikon D70s camera. The quality achieved with these cameras is consistently high, in this case coping well with moderate lenticular haze. |
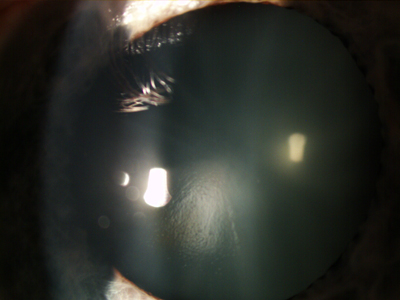
Routine Digital Anterior Imaging (DAI)
This image is simply that. A quick routine capture with one of our Topcon SC-D7 Biomicroscopes fitted with a DW3 camera. The focal plane is the anterior lens surface, and illumination is arranged simply to demonstrate the degree of lenticular haze present. When performed routinely, the practitioner quickly learns to accurately assess the correlation between DRI image quality and lenticular haze or cataract, and in turn how this might translate to the Patient's acuity. This then becomes useful when trying to assess how much acuity reduction might be due to the degree of Cataract present and how much might be attributable to ARMD. But we digress ........
|
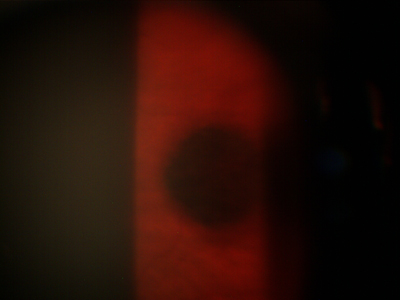
Routine Indirect Ophthalmoscopy by Volk
No other measurement, and no other part of the examination revealed anything other than normal results. This capture was achieved with a 78D Volk lens and 16x magnification on a Topcon SL-D7/DW3. This really brings home a number of points. Firstly, how dangerous it would be to rely solely on a single central 45 degree field of two dimensional DRI image in routine eye examination. Secondly the simple fact that this lesion would have remained undetected had the patient not been dilated for reason of small pupils. Thirdly, how close this was to being undetected even with a dilated patient, and a conscious effort to "get out there" !! |
DRI Mosaic
This is not something that we would normally routinely do, but here we really just want to consider the field that we can capture in this way, see if our lesion is visible by these means, and establish how much further into the periphery we need to go beyond these limits. Despite a slight darker patch creeping onto the edge of some of these captures, none is our lesion. In fact they are artifacts brought about by a combination of oblique fixation and pupil size. There are many ways to combine images. Here we had no time to blend, and simply stacked the images in a spiral to produce the desired effect. |
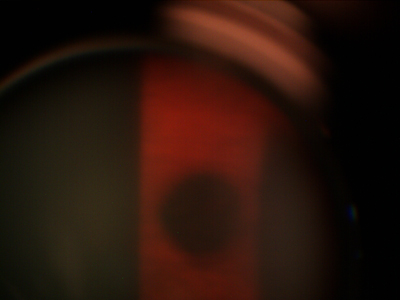
90D Volk - Topcon SL-D7/DW3 - 6x magnification
In order to try to get a better impression of the whole actual outline shape, a reduction of biomicroscope magnification to 6x, and a switch to a 90D Volk lens was used. We are of course at this stage trying to decide, benign neavus or choroidal melanoma. We know that this gentleman has a history of liposarcoma, and although there is really no link in aetiology it is nonetheless very difficult to ignore this simple bit of patient history. |
90D Volk - Topcon SL-D7/DW3 - 16x magnification
We now have a clear idea of shape, and we know that irrespective of any possible referral we want our own record of this lesion for our own future comparison as part of our own clinical care. Shape is fine, but we are still lacking surface detail, and it is clear that this is not going to be achieved in this configuration. |
78D Volk - Topcon SL-D7/DW3 - 16x magnification
It must be pointed out that "human" glimpses of this quality were readily achieved, and of course the 3rd dimension provided by a stereoscopic view is of considerable value in these cases. But in routine practice it is much easier to visualise only part of the lesion, and scan across it as part of the examination. That is fine for diagnostic purposes, but to achieve a similar impression by means of photographic capture is a whole different ball game. A few issues spring to mind as difficulties to overcome. The time delay between pressing the trigger and the actual capture taking place, a lot of movement can occur in that time. What is in focus through the eyepieces is not always exactly in focus to the camera, and while part of this can be dealt with in the setting up of the instrument there is still the need to switch view between eyepiece and screen. Movement within the exposure duration is also a significant problem, and it can be very difficult to eliminate "movement blur". |
ConclusionIn diagnosing this lesion we considered it's shape and it's colour, we decided that it wasn't raised, although the two dimensional perception of blood vessel path might contradict the more reliable three dimensional visualisation. We noted that the edges were well defined but had some pigment variation both at the edges, and indeed across the lesion itself. The surrounding blood vessels appeared normal. There were some small drusen on the lesion, and in particular at the edges. We also considered the possibility of a small area of sub choroidal haemorrhage. We considered the patients past liposarcoma history, and at the same time tried to ignore it ! Naevus or Melanoma ? Melanoma or Naevus ? The problem with this lesion was that it wasn't typical enough of routine naevi to allow sufficient confidence that we could simply review this case after a period of time. We felt that this was deserving of Ophthalmological opinion, but at the same time would schedule our own review. The patient has been seen at hospital level, currently awaits both ultrasound examination and the hospital's own retinal imaging, and is frustrated by the slow pace. It may be that our own follow up may occur before any hospital conclusion, and we are in a good position to provide accurate and reliable assessment of any visual change to this lesion, and hope that this might provide the first stage of ongoing reassurance for this patient. The interesting things about this case are firstly the difficulty in actually viewing this lesion. The quality of the images taken through a Volk lens if they had been more central would perhaps be judged average or even poor, but to acquire any image at all in the extreme periphery, as here, is actually quite an achievement. From a clinical point of view the interesting things are firstly the difficulties of certainty of diagnosis with an unusual combination of features. It also demonstrates nicely the difficulties faced by every working Optometrist every day of life, not to mention the jeopardy involved therein. So what have we learned so far ? ...... Firstly, how easily this might have been missed. Secondly that despite a high level of clinical care, and with the best intentions and the best will in the world, the limitations of an eye examination, the limitations of resources and the limitations of the instrumentation that we have available to us mean that it is inevitable that on occasion some features will remain undetected. Thirdly there is probably a strong argument for the dilation of every patient that walks through our doors. Fourth, .... use all of your instrumentation to best advantage, but never in isolation or as a replacement for an overlapping method. Fifth and finally, .... DRI is probably now pretty commonplace in routine examination, but there is a place and a similar strong justification for routine DAI, as a diagnostic aid, for future comparison, for the ability to actually show the patient what you are talking about, for your own protection and defence in litigation. Daily use of a digital biomicroscope allows not only DAI, but with the use of a Volk lens provides the ability to produce DRI images that are not achievable with a retinal camera. Most importantly this can be part of a drive to continually seek to raise the standard of ongoing clinical care. |